Use of the OTSC®neo System Set
The OTSC®neo System Set is used in flexible endoscopy in the gastrointestinal tract for:
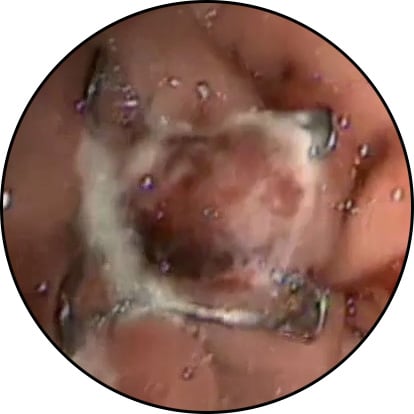
- Compression and tissue approximation
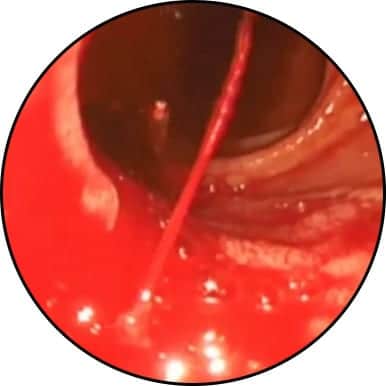
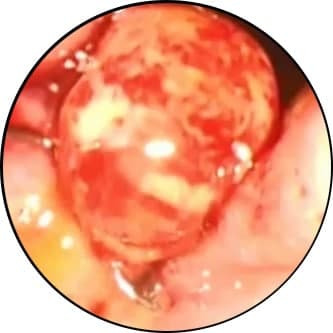
- Hemostasis
- Treatment of gastrointestinal organ wall lesions
The OTSC®neo System Set
The OTSC®neo System Set consists of:
- Applicator cap with a mounted clip made from super elastic Nitinol®
- Thread
- Thread retriever
- Hand wheel for clip release
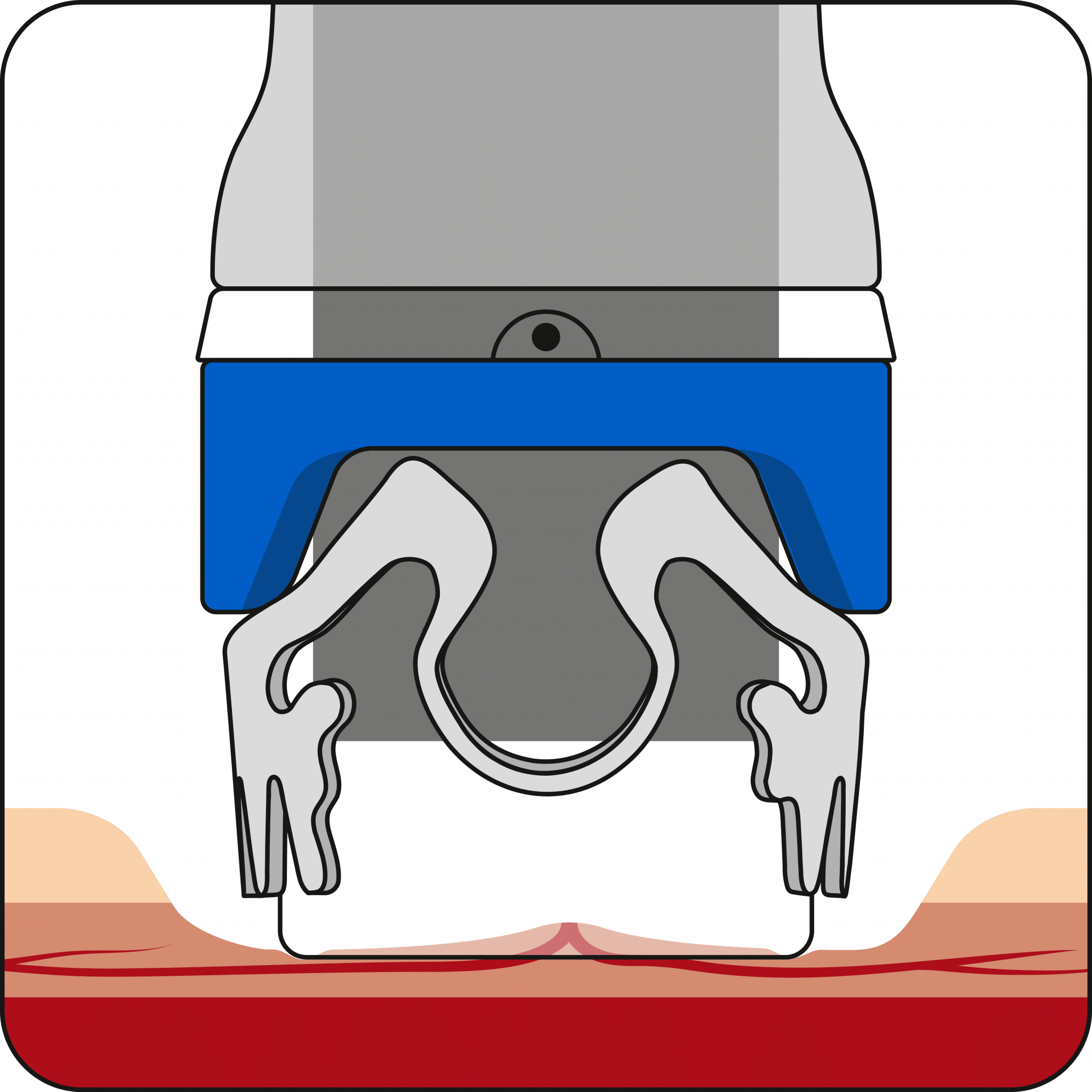
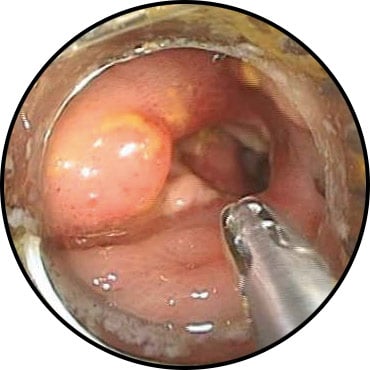
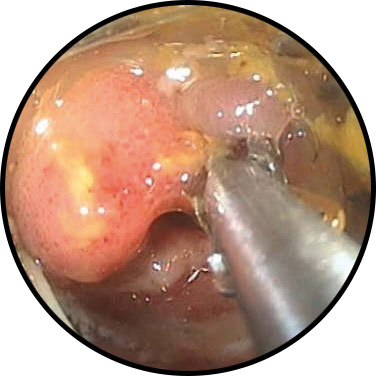
Application
Due to its unique design, the clip closes after application and anchors itself in the tissue. This stops bleeding or closes lesions of an organ wall in the gastrointestinal tract. Due to its smart material properties, the clip delivers a constant force on the tissue securing the therapeutic effect. The clip is made of biocompatible and MR conditional material and can remain in the body as a long-term implant.
*Please refer to the instructions for use and note country-specific approvals and indications.

 Deutsch
Deutsch  Français
Français  Español
Español  Português
Português