Deutsch
Deutsch  Français
Français  Español
Español  Português
Português The colonic FTRD® enables endoscopic full-thickness resection of lesions in the colon and rectum.









+49 (0) 7071 96528 160
service@ovesco.com
Instrument for flexible endoscopy, for full-thickness resection and diagnostic tissue acquisition through removal of suitable lesions in the colorectum.
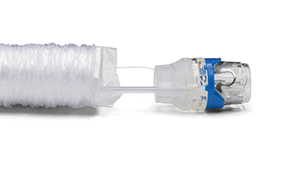
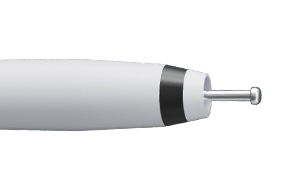
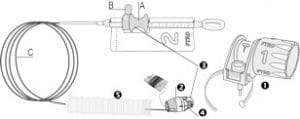
The colonic FTRD® consists of an applicator cap with a ready-to-use mounted FTRD® clip, integrated HF snare and thread. Included are the thread retriever for easy retrieval of the release thread, the endoscope sleeve with fixation tapes and FTRD® hand wheel.
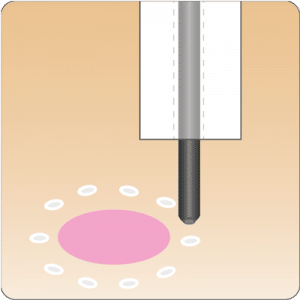
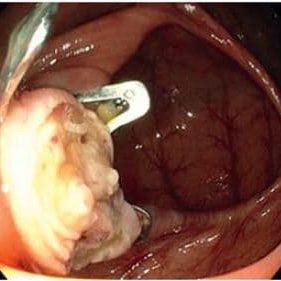
For application, the applicator cap is mounted on the endoscope with the snare running on the outside of the scope and the sleeve preventing entrapment of any tissue between scope and snare. By turning the hand wheel, the thread is tensioned and the clip released. Using the integrated snare, the target tissue is cut above the clip.
The size of the colonic FTRD® is suitable for endoscopes with a diameter of 11.5 - 13.2 mm and a working channel diameter of at least 3.2 mm.
The colonic FTRD® is delivered as one procedure set and consists of the following products:
Before purchasing and using the FTRD®, participation in a training course is mandatory.

| Cap diameter (outside) [b] | 21 mm |
| Cap diameter (inside) [c] | 13 mm |
| Cap depth | 23 mm |
| Appropriate endoscopes | Endoscope diameter: 11.5 - 13.2 mm Working channel diameter: min. 3.2 mm |
| Packaging unit | 1 piece included in colonic FTRD® Set |
| Reference number of the colonic FTRD® Set (incl. FTRD® Marking Probe und FTRD® Grasper) | 200.70 |
The colonic FTRD® is compatible with all commercially available colonoscopes. All FTRD® products are disposable and designed for single patient use.
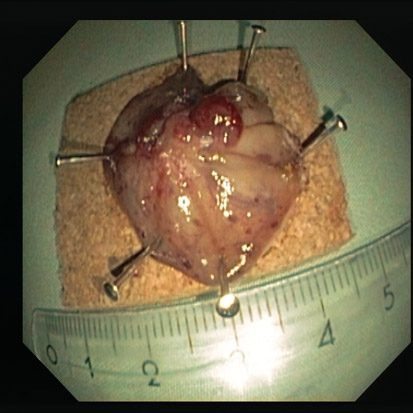
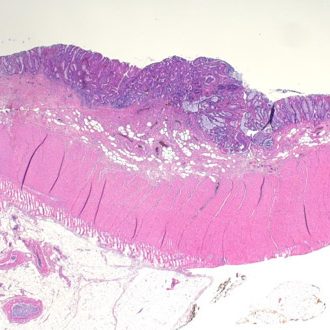
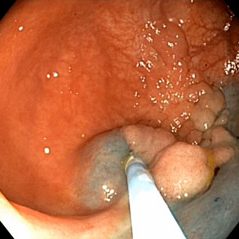
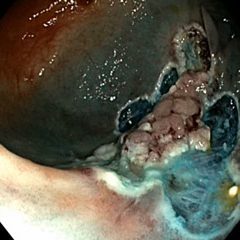
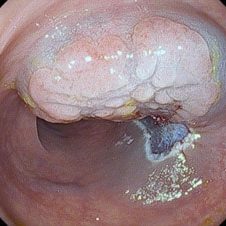
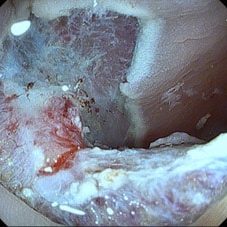
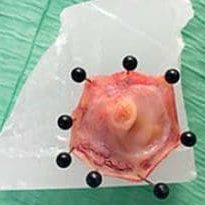
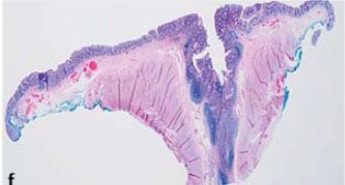
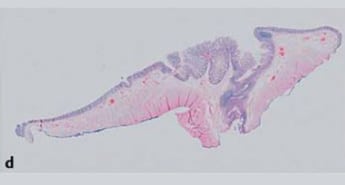
Procedural sequence EFTR of a recurrent sessile adenoma (non-lifting sign) in the descending colon

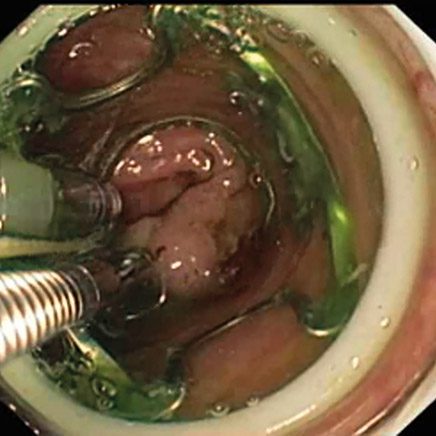

* Source: Prof. K. Caca and Dr. A. Schmidt, Klinikum Ludwigsburg, Dept. of Internal Medicine, Gastroenterology, Hemato-Onkology, Diabetes and Infektious Diseases, Germany
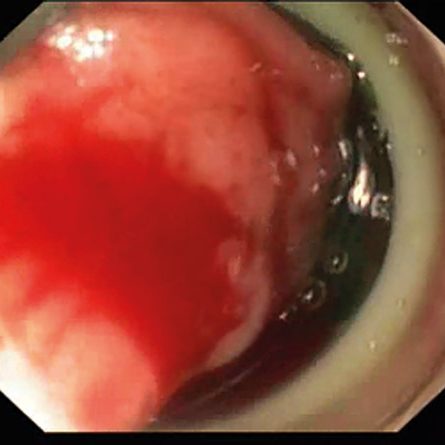
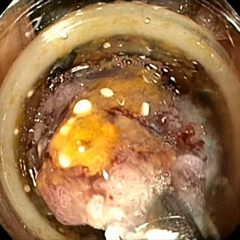
De novo resection after incomplete polypectomy in the descending colon (early carcinoma)



* Source: Prof. K. Caca and Dr. A. Schmidt, Klinikum Ludwigsburg, Dept. of Internal Medicine, Gastroenterology, Hemato-Onkology, Diabetes and Infektious Diseases, Germany
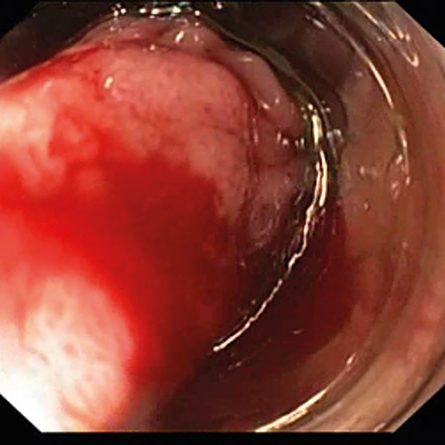
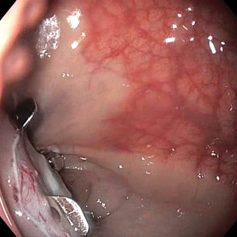
Resection of a relapsed adenoma (HGIEN) in the descending colon (non-lifting sign)


* Source: Prof. K. Caca and Dr. A. Schmidt, Klinikum Ludwigsburg, Dept. of Internal Medicine, Gastroenterology, Hemato-Onkology, Diabetes and Infektious Diseases, Germany
Animation of the Hybrid-FTRD® procedure
Resection of a recurrent sigmoidal adenoma with the Hybrid-FTRD® technique – (Click here to see the corresponding clinical video)


* Source: Prof. K. Caca and Dr. B. Meier, Hospital Ludwigsburg, Germany
Resection of a large cecal adenoma with the Hybrid-FTRD® technique – (Click here to see the corresponding clinical video)



* Source: Prof. K. Caca and Dr. B. Meier, Hospital Ludwigsburg, Germany
Resection of an approx. 35 mm large non-lifting adenoma (LST granular type) in the sigmoid colon; Follow-up after 3 months without recurrence
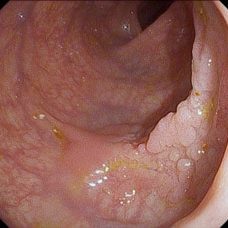


* Source: Dr. M. Bauermeister, Sana Klinikum Lichtenberg Berlin, Germany
Resection of an approx. 25 mm large non-lifting recurrent adenoma (LST granular type) in the upper rectum




* Source: Dr. M. Bauermeister, Sana Klinikum Lichtenberg Berlin, Germany
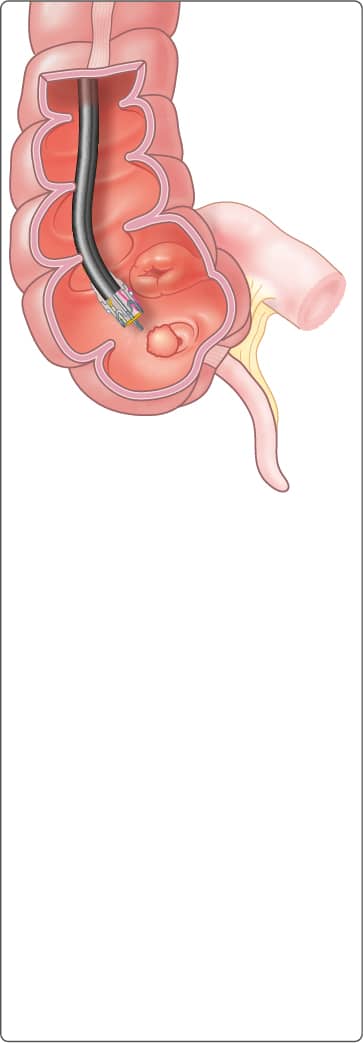
Schematic illustration oft he EFTR procedure of a polyp involving the appendiceal orifice.
* Source: Rogier Trompert Medical Art, www.medical-art.nl
The procedure is presented here in animated form




* Source: Bronzwaer M, Bastiaansen B, Koens L et al. Endoscopic full-thickness resection of polyps involving the appendiceal orifice: a prospective observational case study. Endosc Int
Open 2018; 06: E1112–E1119
Prof. K. Shishin MD, Moscow Clinical Research Center, Russia
Click here to see the clinical video
Dr. B. Bastiaansen, UMC Amsterdam, Netherlands
Click here to see the clinical video